This blog post came out of my quest for finding a medical explanation/term for my own pain caused by dietary oxalates and a desire to gain a better understanding for my clients who experience similar pain. It’s been on my writing list for some time and I’ve been gathering articles and research but the current coronavirus pandemic and recommendations for high vitamin C intake had me concerned enough to blog about it and ask for feedback from my community.
This is the blog, Coronavirus and vitamin C for immune support: new pain or more severe pain due to oxalate issues?, where I pose the question about recent increased intake of vitamin C or the addition of large doses for immune support and increased pain: joint pain, eye pain, foot pain, vulvodynia, bladder issues, insomnia, gut pain, kidney pain, changes in thyroid health/labs, bone pain etc? The feedback on this blog and on Facebook has been huge and confirms the connection. Thank you if you’ve already contributed to the discussion!
Today I’ll share an overview of oxalates, my pain issues with dietary oxalates, a deeper dive into the condition called oxalate crystal disease (with some of my insights and questions), and the autism and atherosclerosis research. It’s by no means a comprehensive blog on all things oxalates but rather a way to try and connect some dots and pose some questions for going deeper.
The next blog will address my vitamin C/oxalate/pain story and the research on vitamin C, oxalates and pain, together with questions.
Oxalates defined and food sources
Before we review oxalate crystal disease, let’s define calcium oxalates. Julie Matthews, my good friend and colleague and an oxalate expert shares this in her blog, Oxalates: Their Influence on Chronic Disease
Oxalates present in our body as sharp crystals or crystalline structures with jagged edges that cause pain, irritation, and distress. They can bind with certain minerals; particularly calcium and magnesium, as well as iron and copper
You’ll find many different lists of low, medium and high oxalate foods. When I started eating low oxalate I found Susan Owen’s site simple and very helpful. I then joined the Trying Low Oxalates Facebook group for support and feedback.
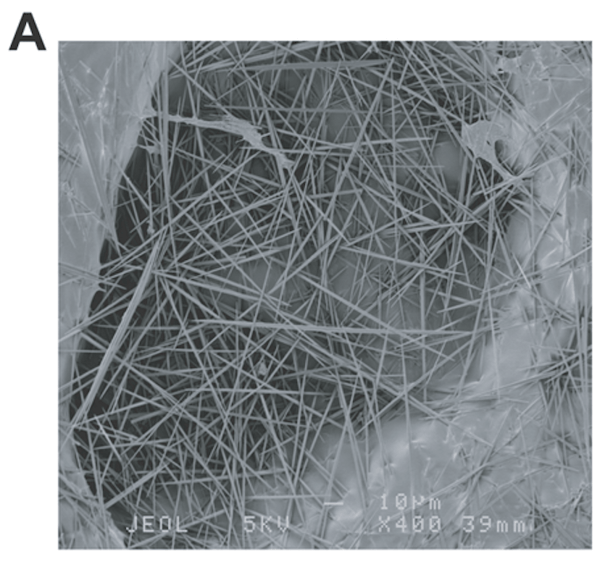
In summary, these are the common medium-oxalate and high-oxalate foods that many folks have problems with: nuts, nut-butters and nut-flour (something to watch when eating Paleo or GAPS), wheat, chocolate, kiwi fruit (very high – see the raphides image below), star fruit (also very high), beets, potatoes, legumes, berries, spinach and soy.
You can see why these needle shaped calcium oxalate crystals found in kiwi fruit could inflict pain. This is just one example – there are many different shapes of calcium oxalate crystals.
My oxalate story: severe foot pain and eye pain
I personally had severe dietary oxalate issues in 2012 which manifested as excruciating foot pain. It was a combination of hot-burning-coals-pain and shards-of-glass-pain. It was just after my book, The Antianxiety Solution (my Amazon link), came out. Due to my book tours and events, I would be on my feet all day presenting, often for 3 full consecutive days, so I figured that must be the reason. When I travelled, I took a blender and made smoothies with berries, ate plenty of healthy nuts as my snacks and took kale chips with me to make sure I was getting my greens. Kiwi fruit was a favorite of mine!
I was eating a high oxalate diet and had no idea until I heard Julie present at an Integrative Medicine for Mental Health Conference on dietary oxalates and autism. A light-bulb went off and then I worked with her to learn about oxalates and figure out if it was in fact because of oxalates and sure enough, as soon as I removed high and medium oxalate foods the pain resolved. Note: the advice is NOT to remove all high and medium oxalate foods at once because dumping can occur. I was fortunate that this didn’t happen with me, possibly because of the vitamin B6 I was already taking as part of the pyroluria protocol.
When I eat a low oxalate diet I do really well. However, more recently dietary oxalates have been causing me eye pain when I have a treat like eggplant or carob. It starts out as a kind of scratchy discomfort and mild pain and then gets worse and worse. I also have a goopy kind of discharge from the inner part of my eye and burning/redness crystal-like teariness on the outer parts of my eyes. I recently had one very severe incident where the eye pain in my left eye was agonizing for about 2 hours. I was beside myself and tried GABA, DPA and tryptophan for an attempt at pain relief – with no success. When I took 500mg of vitamin B6 the pain eased immediately.
The theory is that oxalates cause issues where you have a weakness. I injured my left eye walking into a low tree-branch while rock-climbing 15 years ago, so I suspect this is why my left eye is more severely affected.
Oxalate crystal disease
The condition “oxalate crystal disease” is the closest explanation I’ve found that explains the pain I’ve experienced and makes the most sense, other than the fact that all the studies mention kidney disease and yet I don’t have kidney disease and have never had kidney stones. I’ve also never had a problem with my estimated Glomerular Filtration Rate (eGFR). In case eGFR is new to you it measures how well your kidneys filter the wastes from your blood and is the best overall measure of kidney function/damage.
This paper, Update on oxalate crystal disease, summarizes it:
Oxalate arthropathy is a rare cause of arthritis characterized by deposition of calcium oxalate crystals within synovial fluid. This condition typically occurs in patients with underlying primary or secondary hyperoxaluria. Primary hyperoxaluria constitutes a group of genetic disorders resulting in endogenous overproduction of oxalate, whereas secondary hyperoxaluria results from gastrointestinal disorders associated with fat malabsorption and increased absorption of dietary oxalate. In both conditions, oxalate crystals can deposit in the kidney leading to renal failure. Since oxalate is primarily renally eliminated, it accumulates throughout the body in renal failure, a state termed oxalosis. Affected organs can include bones, joints, heart, eyes, and skin. Since patients can present with renal failure and oxalosis before the underlying diagnosis of hyperoxaluria has been made, it is important to consider hyperoxaluria in patients who present with unexplained soft tissue crystal deposition. The best treatment of oxalosis is prevention. If patients present with advanced disease, treatment of oxalate arthritis consists of symptom management and control of the underlying disease process.
Let me break this down because I’ve had to look up terminology and read and re-read papers in order to get a better understanding of things:
#1 Oxalate arthropathy is a rare cause of arthritis characterized by deposition of calcium oxalate crystals within synovial fluid.
Oxalate arthropathy is a disease of the joints caused by oxalates depositing in the synovial fluid of the joints. The paper states it is a rare cause of arthritis, but I suspect it is much more common given what we’re seeing clinically.
Also, because all the research connects oxalate crystal disease with kidney disease, it may be overlooked when there is no kidney disease (more on that below).
Synovial fluid is the fluid between the joints that acts as a lubricant and nutrient source.
#2 This condition typically occurs in patients with underlying primary or secondary hyperoxaluria.
Hyperoxaluria occurs when you have “too much oxalate in your urine.”
#3 Primary hyperoxaluria constitutes a group of genetic disorders resulting in endogenous overproduction of oxalate and… secondary hyperoxaluria results from gastrointestinal disorders associated with fat malabsorption and increased absorption of dietary oxalate.
Primary hyperoxaluria is genetic and results in endogenous or internal overproduction of oxalate, causing too much oxalate in the urine.
The secondary hyperoxaluria description mentions “gastrointestinal disorders associated with fat malabsorption and increased absorption of dietary oxalate.” There are a number of other factors which I’ll address in a future blog.
According to this paper and others, secondary hyperoxaluria also results in too much oxalate in the urine.
#4 In both conditions, oxalate crystals can deposit in the kidney leading to renal failure. Since oxalate is primarily renally eliminated, it accumulates throughout the body in renal failure, a state termed oxalosis.
Affected organs can include bones, joints, heart, eyes, and skin.
Mayo clinic states oxalosis occurs if your kidneys fail. “Because your body can no longer eliminate the extra oxalate, it starts accumulating — first in your blood, then in your eyes, bones, skin, muscles, blood vessels, heart and other organs.”
My comment is that in some instances, oxalates accumulate in various parts of the body without kidney failure. I share more about this aspect and what we see clinically below, plus an autism and atherosclerosis study.
This paper, Oxalate crystal deposition disease, also mentions the following: “osteopathy, acute and chronic arthropathy with chondrocalcinosis, synovial calcification, and miliary skin calcium oxalate deposits and vascular calcifications that affect mainly the hands and feet.” The paper is focused on primary hyperoxaluria (and does also discuss the kidney involvement) but I’m including it because of the conditions listed. You may have received one of these diagnoses and not linked it back to dietary oxalates and/or vitamin C intake possibly playing a role.
The authors do report “systemic life-threatening cardiovascular, neurologic, and hematologic manifestations”, saying they are rare.
Calcium oxalates: anxiety, sleep, headaches, fatigue and other symptoms
Calcium oxalate crystals can also be found in the thyroid, and ear, leading to hearing loss under some circumstances.
Julie Matthews, in her blog, Oxalates: Their Influence on Chronic Disease, also shares that
Clinical studies and anecdotal experience indicate that oxidative stress, mitochondrial disruption and damage, and nutrient depletions, trigger widely varied symptoms including fatigue and inflammatory cascades, joint pain or pain anywhere in the body. Chronic low energy is very common because of a reduction in ATP in the mitochondria. Oxalates could be a hidden source of headaches, urinary pain, genital irritation, joint, muscle, intestinal or eye pain.
Other common oxalate-caused symptoms may include mood conditions, anxiety, sleep problems, weakness, or burning feet. Indicators can be digestive, respiratory, or even bedwetting for children.
What the researchers are saying – always kidney disease
I’ve reached out to a number of researchers, practitioners and labs and they all state that oxalate crystal disease only happens with kidney disease/kidney stones. This is what one researcher shared with me: “Plasma oxalate concentrations only elevate enough to cause systemic disease when there is significant kidney disease (typically GFR <20-30). I have never seen a significantly elevated plasma oxalate without chronic kidney disease.”
Could this be the case because they are kidney specialists and therefore only seeing patients who already have kidney disease?
The good news is that a number of them are intrigued and interested in learning more.
Oxalate crystals in autism and atherosclerosis without kidney issues
However, based on my own experience and according to many in this community and other communities like the Trying Low Oxalates Facebook group, pain issues related to dietary oxalate intake may occur without kidney issues/kidney stones, and often does.
These papers offer some support for what I suspect we are seeing clinically – systemic oxalate deposits can occur deposits without kidney stones or renal failure:
Children with ASD [autism spectrum disorder] demonstrated 3-fold greater plasma oxalate levels … and 2.5-fold greater urinary oxalate concentrations. Despite significant hyperoxaluria no evidence of kidney stone disease…was observed
calcium oxalate crystals were observed within atherosclerotic plaques in the coronary arteries. Similar deposits were seen in the thyroid gland and other organs but not in the kidneys. None of the patients had chronic renal failure…. We suggest the phrase “atherosclerotic oxalosis” to describe this finding.
These are the disconnects I’m seeing in the research and questions I have:
- Oxalate crystal disease is reported to be rare and it only happens with kidney disease/kidney stones – could it be more common than reported? As Julie states: “New science and clinical experience reveal concerns about oxalates that far exceed traditional kidney stone pathology.”
- Should we be calling it hyperoxaluria. “too much oxalate in your urine” if the kidney is not involved? Or do we need to expand the definition of hyperoxaluria to include too much oxalate in other tissues outside the kidney and urine?
- Could oxalate crystal disease with no kidney disease be a new syndrome that has yet to be widely and clearly identified in the research?
I mean no disrespect to the study authors and researchers by sharing my insights and questions here and in the section above. I appreciate the work they do and the opportunity to learn from them.
Searching through the literature on this has been extremely challenging because studies always refer to the kidney. It may well be that there is a perfectly logical explanation for much of this and someone has already gone through the research and has answers to all my questions. I am very willing to be enlightened so please do share if you’ve come across a good explanation.
Either way, please share your insights based on what I’ve shared in this blog and in relation to your experiences with pain caused by dietary oxalates and/or pain caused by vitamin C intake. I will be sharing this blog and the comments with the researchers and practitioners who are open to all this.
Read all posts in this series:
- Coronavirus and vitamin C for immune support: new pain or more severe pain due to oxalate issues? (part 1)
- Oxalate crystal disease, dietary oxalates and pain: the research & questions (part 2)
- Vitamin C causes oxalate formation resulting in pain, anxiety, and insomnia (when there is a defect in ascorbic acid or oxalate metabolism)? (part 3)
- Willow’s survival story: Easter Lilies cause acute renal failure in cats and Peace Lilies cause oxalate issues (part 4)
- Waking in the night due to environmental toxins: impacts on the liver, gallbladder and fat digestion (making oxalate issues worse) (part 5)
- Increased kidney stones in postmenopausal women with lower estradiol levels. What about increased dietary oxalate issues too?
- Vulvodynia: oxalates, GABA, tryptophan and physical therapy